

The Hormonal Dermal Axis.
Polycystic Ovary Syndrome (PCOS) is a systemic endocrine disorder with a profound dermatological footprint. In the Indian phenotype, insulin resistance and androgen excess manifest as a Clinical Triad of hormonal acne, acanthosis nigricans, and follicular miniaturization. Understanding these signals is the first step toward metabolic and dermal recovery.
The Systemic Signals
PCOS-Related Dermatology
Polycystic Ovary Syndrome (PCOS) is not merely a reproductive concern; it is a systemic endocrine disorder that manifests significantly through the skin. In the Indian context, where genetic predispositions to Insulin Resistance are high, the dermatological symptoms of PCOS often serve as the first clinical “red flags.”
The PCOS-Dermal Correlation (2026 Metrics)
Of women with PCOS exhibit **Insulin Resistance**, the primary driver behind Acanthosis Nigricans (darkened skin folds) and skin tags.
The specific anatomical distribution (Jawline/Chin) where **80% of hormonal acne** manifests, distinguishing it from digestive or hygiene-related breakouts.
The window required for clinical **Androgen Suppression** to show visible reduction in new hirsutism growth or scalp hair recovery.
1. The Hyperandrogenism Trigger
At the core of PCOS is an excess of androgens (male hormones). In the skin, these hormones act as a “volume knob” for the sebaceous glands.
-
The Sebum Surge: Androgens stimulate the oil glands to produce a thicker, more wax-like sebum. When this combines with Delhi’s high particulate matter (PM2.5), it creates a “plug” that is far more difficult to treat than standard teenage acne.
-
Hormonal Acne Geography: PCOS-related acne typically follows a “U-zone” pattern—concentrating along the jawline, chin, and neck. These are often deep, painful cystic lesions that leave behind significant Post-Inflammatory Hyperpigmentation (PIH).
2. Insulin Resistance & Acanthosis Nigricans
A highly searched but often misunderstood symptom in India is Acanthosis Nigricans (AN). Many patients mistake this for “dirt” or simple tanning.
-
The Biological Mechanism: High levels of insulin in the blood accidentally trigger IGF-1 receptors in the skin. This causes a rapid, abnormal growth of keratinocytes (skin cells) and fibroblasts.
-
The Presentation: The skin becomes “velvety,” thickened, and dark, primarily around the neck, armpits, and groin. This is a direct dermal reflection of internal metabolic stress and cannot be “scrubbed” away; it requires clinical management of the insulin-skin axis.
3. Uncommon Sub-Topic: “The PCOS Hair Paradox”
One of the most distressing aspects of PCOS is that it causes hair to grow where it isn’t wanted and fall out where it is.
-
Hirsutism (Excess Growth): Androgens convert fine, vellus hair into thick, terminal hair on the face, chest, and back. This is why Diode Laser Hair Removal is a cornerstone of PCOS management—not just for aesthetics, but for the psychological well-being of the patient.
-
Female Pattern Hair Loss (FPHL): While facial hair increases, the scalp hair follicles “miniaturize” due to DHT sensitivity. This leads to a visible widening of the hair part.
Decoding the Dermal Conversions
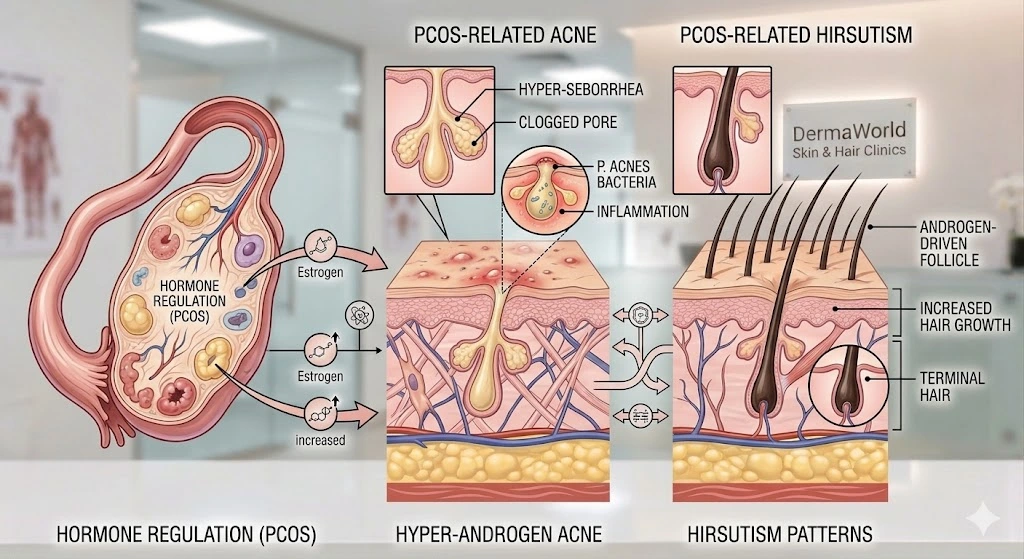
This detailed visual (right) provides a definitive anatomical roadmap, clarifying how hormonal dysregulation is not an abstract concept, but a direct physical transformation of the dermal architecture. While general PCOS summaries exist, we must analyze the specific three distinct biological ‘conversions’ shown, as they dictate the required clinical response for Indian phenotypes.
1. Hormone Regulation (The Source): The visual clarifies the ovarian Androgen Surge that overrides normal checks and balances.
2. Hyper-Androgen Acne: We decode the Hyper-Seborrhea and Clogged Pore cascade that leads to deep-pore P. acnes (Propionibacterium acnes) proliferation.
3. Hirsutism Patterns: The illustration confirms how DHT sensitivity converts fine ‘Vellus’ hair into thick, dark ‘Terminal’ hair.
Visualized Endocrine-Dermal Axis Cascade (2026)
The “PCOS-Dermal Axis” Breakdown
In modern trichology, we must analyze the Androgen-Driven Follicle specifically within the PCOS environment. The high-mineral content common in Indian tap water (calcification) can exacerbate the brittle nature of hair shafts weakened by DHT.
This image provides a definitive anatomical roadmap, illustrating how hormonal dysregulation is not an abstract concept, but a direct physical transformation of the dermal architecture. By analyzing the three distinct panels, we can decode the entire biological cascade.
[Image showing the full PCOS endocrine-dermal cascade, including hormone regulation, hyper-androgen acne, and hirsutism patterns]
Decoding the Three Dermal Conversions
-
Hormone Regulation (The Source): The left panel of the visual clarifies the primary endocrine shift. While Estrogen levels may appear normal or slightly high, it is the sharp, unregulated increase in Androgen production from the ovary that is the systemic critical point. This “Androgen Surge” overrides the skin’s normal checks and balances.
-
Hyper-Androgen Acne (Panel 2): As shown in the center panel, the excessive androgens stimulate the sebaceous glands to enter a state of Hyper-Seborrhea. This sebum is not only plentiful but also thicker. When it mixes with atmospheric pollution, it quickly forms a Clogged Pore. The visual confirms that this creates the perfect, low-oxygen environment for P. acnes (Propionibacterium acnes) bacteria, leading to the deep, painful Inflammation characteristic of cystic PCOS Acne.
-
Hirsutism Patterns (Panel 3): The right panel illustrates the distressing condition of PCOS Hirsutism. Under normal circumstances, vellus (fine) hair covers much of the body. In PCOS, the terminal hair follicles in specific anatomical regions (like the jawline and chin) are DHT-sensitive. This hormonal shift creates an Androgen-Driven Follicle, which converts fine, vellus hair into thick, dark, and deep-rooted Terminal Hair, requiring targeted clinical destruction.