


Dermatology in the Indian Context: A Specialist’s Overview
Dermatology is the branch of medicine focused on the integumentary system—the complex biology of the skin, hair, and nails. In the diverse Indian landscape, dermatology transcends aesthetics; it is a vital clinical intervention for maintaining systemic health against a backdrop of extreme UV indices, fluctuating humidity, and urban particulate matter (pollution).
The Evolution of Skin Science in India
India’s relationship with dermatology is a synthesis of ancient observational wisdom and modern molecular science.
-
Heritage: Early Ayurvedic texts like the Charaka Samhita first identified inflammatory skin conditions, utilizing botanical stabilizers like Neem and Turmeric.
-
Modernity: Today, the field has evolved into a high-tech discipline. From treating recalcitrant tropical infections to performing micro-surgical hair transplants in metros like Delhi and Mumbai, Indian dermatology is now a global benchmark for treating melanin-rich skin types.
Clinical Benchmarking & Rigor
Standard Indian Pathway
- Step 1: MBBS (5.5 Years) Core medical foundation from an NMC-recognized institution.
- Step 2: NEET-PG Qualification Competitive national entrance for specialized residency.
- Step 3: MD/DNB Specialization (3 Years) Intensive focus on the 3,000+ pathologies of skin, hair, and nails.
- Step 4: NMC Licensure Final inclusion in the National Medical Register for legal practice.
Foreign Medical Graduates
Specialists educated abroad (UK, USA, Australia, etc.) must complete the NMC Equivalency Protocol to ensure clinical parity with Indian standards.
🛡️ FMGE / NExT Validation
Mandatory clearance of national qualifying exams to verify clinical competency.
🛡️ Supervised Internship
12-month local hospital rotation to adapt to regional skin pathologies.
Common Dermatological Pathologies in India
The Indian climate acts as a primary trigger for specific skin and scalp conditions. Understanding these “curveballs” requires a specialist’s diagnostic eye.
| Clinical Condition | Environmental/Biological Driver | The Dermatologist’s Approach |
|---|---|---|
| Acne Vulgaris | Sebum overproduction + Humidity | Targeted hormonal & topical regulation. |
| Melasma | UV Exposure + Hormonal triggers | Enzymatic Tyrosinase Inhibition (Cosmelan). |
| Tinea (Fungal) | High Humidity & Perspiration | Steroid-Free antifungal protocols. |
| Alopecia | Pollution + Hard Water + Stress | PRP, GFC, and FUE Transplant interventions. |
| Psoriasis | Autoimmune + Dry Winter Triggers | Biologicals and localized stabilization. |
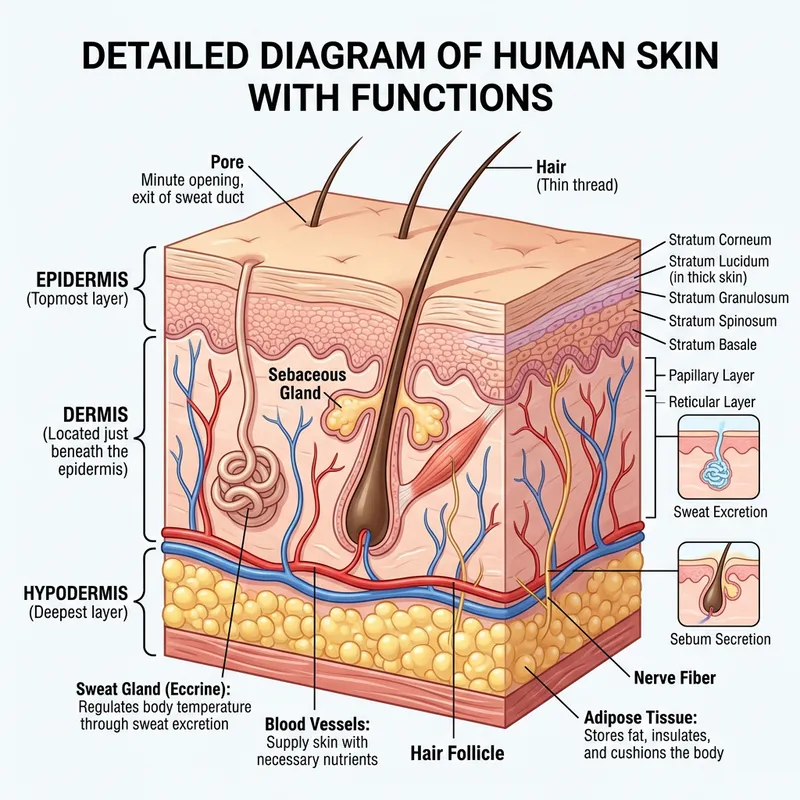
Dermal Architecture: The Fitzpatrick Matrix
Indian skin possesses a higher density of eumelanin, providing natural photoprotection but increasing the risk of Post-Inflammatory Hyperpigmentation (PIH).
Specialist assessment reveals a thicker dermis in Indian phenotypes, which provides a resilience against fine lines but requires targeted energy for deep cystic acne.
Fluctuating humidity triggers rapid barrier disruption. Professional “Medical Moisturization” stabilizes this barrier better than standard over-the-counter lotions.
Clinical Triage Scale
Dermal Ethnography
1. The “Steroid-Induced” Epidemic
A Silent Indian Crisis
The Gap: Millions of Indians use over-the-counter “fairness” or “anti-itch” creams (often containing Clobetasol or Betamethasone) without realizing they are damaging their skin DNA.
In the Indian pharmaceutical landscape, the ease of access to high-potency steroid cocktails has led to a clinical crisis. At DermaWorld, we frequently treat Topical Steroid Damaged Face (TSDF). Chronic use of these ‘quick-fix’ creams causes irreversible skin thinning (atrophy), telangiectasia (visible blood vessels), and a specialized form of ‘rebound’ redness.
A dermatologist’s role in India is often as much about ‘Skin Detoxification’ as it is about treatment. We transition patients from steroid dependence to medical-grade stabilizers that restore the basement membrane without triggering inflammatory flares.
2. The AQI-Aging Correlation
(Urban Dermal Stress)
The Gap: Most people think pollution just causes “dirt.” Clinically, PM2.5 particles are small enough to enter pores and trigger oxidative stress that mimics sun damage.
Living in a high-AQI environment like Delhi-NCR or Mumbai is equivalent to constant ‘Extrinsic Aging.’ Particulate matter (PM2.5) acts as a catalyst for lipid peroxidation, which destroys the skin’s natural moisture barrier. Data suggests that urban residents in India experience a 15-20% faster degradation of Type I Collagen compared to those in cleaner air zones.
This manifests as ‘Urban Grayness’ and premature sagging. Our dermatological approach involves ‘Atmospheric Protection’—utilizing chelating agents and powerful antioxidants like Vitamin C and Ferulic Acid to neutralize heavy metal deposits on the skin surface.
3. Tropical Trichology
Why Indians Lose Hair Differently
The Gap: Hair loss in India is rarely just “genetic.” It is heavily influenced by “Hard Water” (high TDS levels) and the “Sweat-Sebum” cycle of the Monsoons.
Trichology in India must account for the ‘Hard Water Factor.’ High concentrations of Calcium and Magnesium in tap water lead to mineral buildup on the hair shaft, causing ‘Weathering’ and breakage.
Furthermore, the high humidity of the Indian Monsoon triggers Seborrheic Dermatitis (dandruff), which, if left untreated, leads to micro-inflammation around the follicle and subsequent shedding. Understanding the difference between Telogen Effluvium (stress-induced shedding) and Androgenetic Alopecia (pattern baldness) in the context of the Indian diet—often deficient in Vitamin B12 and Ferritin—is the key to successful hair restoration.”
4. Nutri-Dermatology
The Glycemic Index of Indian Diets
The Gap: The link between high-carb Indian diets (white rice, refined flour, sugar-heavy snacks) and adult acne/PCOS-related skin issues. The ‘Acne-Diet’ connection is scientifically verified in the Indian context.
Diets high in High-Glycemic Index (GI) foods—such as refined flour and sugars—trigger a spike in Insulin-like Growth Factor 1 (IGF-1). This hormone signals the sebaceous glands to produce more oil, leading to persistent adult acne. Furthermore, the Indian prevalence of Insulin Resistance often manifests on the skin as Acanthosis Nigricans (dark, velvety patches on the neck).
A dermatologist in India doesn’t just prescribe topicals; we perform a metabolic audit to ensure your skin health is being supported by your internal biochemistry.
Climate-Adaptive Dermatology Protocol
Seasonal adjustments optimized for North Indian environmental triggers.
Peak Summer (April – June)
- Focus: Photoprotection & Sebum Control.
- Risks: Solar Lentigines, Polymorphic Light Eruption.
- Protocol: High-SPF Physical Blockers & Salicylic Peels.
Monsoon (July – Sept)
- Focus: Antifungal Prophylaxis.
- Risks: Recalcitrant Tinea, Folliculitis, Humidity-Acne.
- Protocol: Steroid-Free Antimycotics & pH Balancing.
Winter (Oct – March)
- Focus: Barrier Repair & Lipids.
- Risks: Xerotic Eczema, Psoriasis Flares, AQI-Pollution damage.
- Protocol: Ceramide-Rich Emollients & Laser Toning.
AQI & Skin: The Invisible Stressor
In high-pollution zones like Delhi-NCR, particulate matter (PM2.5) is small enough to penetrate the skin barrier, triggering chronic oxidative stress. This leads to “Pollution-Induced Pigmentation” and the premature breakdown of collagen.
Our clinical approach focuses on neutralizing these toxins using antioxidant-rich medical facials and restorative laser therapies that reboot the skin’s natural defense mechanisms.
Diagnostic Fact
“Long-term exposure to high AQI levels is clinically linked to a 20% increase in facial pigment spots and a significant reduction in skin hydration levels.”
Bridging Diagnostic Science with Specialized Care
Effective resolution of complex skin, hair, and nail concerns requires more than just a general understanding—it demands a precise, physician-led intervention. Our clinical ecosystem is designed to translate dermatological research into personalized treatment paths, ensuring every patient receives a gold-standard experience calibrated to their unique biological profile.
Perfect Blend of Medical & Cosmetic Dermatology
Clinical Dermatology
We specialize in the diagnosis of chronic and acute conditions. From managing persistent adult acne to complex cases like Psoriasis and Vitiligo, our approach is rooted in “Zero Guesswork.”
Dr. Rohit Batra ensures every treatment is tailored to the unique physiological needs of Indian skin types.
Aesthetic Procedures
We focus on enhancing natural features using Gold-Standard technologies. From HIFU to Botox and Dermal Fillers, our goal is “Aesthetic Confidence.”
Every injection is performed with surgical precision and clinical safety at the forefront.
Adapting to the “Delhi-Mumbai” Climate Rollercoaster
In India, your skincare must be seasonal.
-
Summer/Monsoon: Focus on oil control and fungal prophylaxis.
-
Winter: Focus on barrier repair and lipid-rich moisturization.
-
Year-Round: Broad-Spectrum SPF (30+) is non-negotiable to prevent photo-aging and DNA damage in skin cells.
Finding a Board-Certified Specialist
When seeking a dermatologist in India, prioritize Board Certification and clinical experience. Look for specialists like Dr. Rohit Batra, who bridge the gap between hospital-grade medical dermatology (Sir Ganga Ram Hospital) and state-of-the-art aesthetic clinics (DermaWorld).